When we first heard that our baby might have a cleft lip and palate, we were beyond shocked. Neither Eric nor I had ever met anyone born with a cleft (to our knowledge). I thought it was something that occurred only in third world countries. Commercials for Operation Smile and Smile Train came to mind - how could this be happening to our baby? Did I do something to cause it?
One of the first things I did when I got home was start researching to better understand our diagnosis. We needed to be informed. Perhaps, as I did at first, you know very little about the condition too. There are a number of wonderful resources out there that are great references. I’d like to share some of my findings here.
Did you know…?
Cleft lip and/or palate affects 1 in 700 newborns in the US. It is the most common birth anomaly.
Cleft lip and/or palate is more common in boys than in girls. Cleft palate alone is more prevalent in girls. Some ethnic groups, such as Asians and American Indians, have higher occurrences of clefting. Cleft lip and/or palate occurs in 1 in 1,000 live births of Caucasian babies.
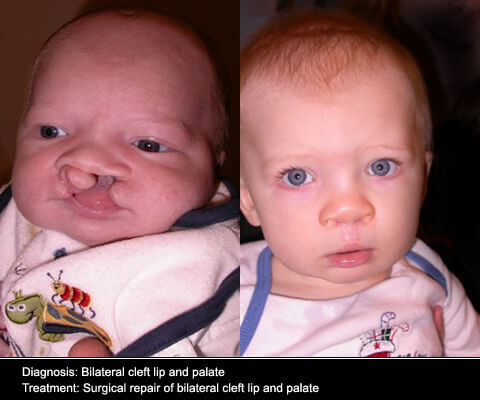
What is a cleft lip or palate?
During the first trimester, the baby’s lip starts to fuse together. Sometimes the lip does not fuse properly and there is a “gap” left. The gap can stretch as far as from the lip to the nostril. A baby can be born with a separation on just one or both sides of the lip (on the left and right).
The palate may also be involved. If the child has a cleft palate it can include both the hard palate (the part that contains bone) the and soft palate (in the back of the mouth). A cleft could occur on one or both sides of the palate too.
Most cleft lips occur in combination with a cleft palate, although sometimes only the lip or only the palate is involved.
What causes a cleft lip or palate?
The cause of clefting is not entirely understood. Family history often plays a role, as well as environmental factors, such as smoking, drinking, and taking certain medications during the pregnancy. The risk of cleft lip/palate increases if the parent or siblings of a baby are also cleft affected. Folic acid deficiency may relate to the cleft. Clefts could be the result of a syndrome. Many times, there is no clear link to its cause.
As far as we know, we have no family history on either side and I have been placing importance on staying healthy and being careful throughout the entire pregnancy. I was taking a prenatal vitamin (with folic acid) before conception and have continued to take it daily.
Why are clefts so unseen in America?
Families in third world countries don’t have access to the medical care and doctors that we have here in the U.S. We often don’t hear about children with clefts because they are repaired so early in life. Over time the scars aren’t as noticeable.
Some cleft affected celebrities include Joaquin Phoenix (microform cleft), Peyton Manning (palate only), and Tom Brokaw.
Does a cleft lip or palate cause a baby pain?
No, clefting does not cause any pain. The baby doesn’t know any differently. Crying, smiling, and other facial movements are not painful for them.
At first, it may be difficult to look at pictures of a baby with a cleft, but please know that they are completely unaware and it does not hurt them.
What challenges does a baby with a cleft face?
While many people believe a cleft lip/palate to be an easy repair, there is a lot more involved than just cosmetic appearance. The most immediate concern for a baby born with a cleft lip and palate is feeding and nutrition. Babies born with a cleft palate have difficulty creating suction - therefore, breastfeeding a baby with a cleft palate is an unlikely scenario. Instead, parents learn to use specialized bottles and nipples that allow them to squeeze pumped milk or formula into the baby’s mouth. Frequent weight checks at the pediatrician are done to ensure baby is gaining weight properly.
Babies born with clefts will need surgery to repair the lip and/or palate. Our baby may have 3 surgeries within his first year of life. The first surgery occurs around 2-3 months. Down the road, as the child continues to develop and grow, other surgeries may be necessary to repair the shape of the nose, revise previous surgeries, and prepare the mouth for permanent teeth to come in.
It is common for babies with cleft palates to have frequent ear infections. A recurring buildup of fluid in the middle ear could cause hearing loss. Tubes are often placed during surgery to help drain the ears and improve hearing. Children with clefts frequently have speech related issues. It is common for them to need speech therapy or even additional surgeries to create normal sounding speech. Children who are cleft affected can have a number of dental abnormalities, as both baby and permanent teeth emerge. Teeth may not come in at the site of the cleft or may come through in unusual places in the mouth. Orthodontic treatment is necessary.
Due to all of these challenges, doctors often work as a multi-disciplinary team to treat babies who are cleft affected. The team may include a plastic surgeon, orthodontist, speech and language pathologist, ENT, audiologist, psychologist, pediatrician, social worker, nutritionist, geneticist, and nurse practitioner.
Another adversity we are preparing for is the acceptance of our child. The advances in medicine and technology are amazing and many times, once the child is older, you can hardly tell that the child ever had a cleft. However each individual handles scarring differently. Particularly, during the school age years, children with clefts are more susceptible to teasing and bullying by their peers.
It is likely that our child will deal with many years of treatment related to his cleft. We are very thankful at how treatable this condition is, but we know it won’t be an easy road. We hope that our journey will bring more awareness to this condition, and along the way, maybe our blog will reach others who are seeking out information and reassurance after receiving a diagnosis of their own. Please feel free to ask us any questions as we continue this learning process.